Why Employee Wellness Programs Don’t Work
The programs focus on individual interventions rather than workload and workplace stress.


October 22, 2024
By Don Sapatkin

Good Tuesday morning! In today’s Daily: We know that workplace wellness programs don’t provide much benefit – but why? And if they don’t work, what could replace them? Plus: In Africa, it’s tough to get mental health care just about everywhere, but good luck getting it from your employer. Ozempic just might, possibly, be a breakthrough drug – for addiction. And bystander administration of Narcan soars.
And for your Tuesday bonus: Gamers say that “cozy” games like Animal Crossing, Unpacking and Stardew Valley – which often feature relaxing tasks, appealing characters and more creative control for players compared with traditional games. − help with their mental health, the BBC reports.
Why employee wellness programs don’t work – and alternatives that might

I remember how surprised I was upon reading a study a few years ago – now one of several – showing that ubiquitous workplace wellness programs don’t provide much benefit. Perhaps I shouldn’t have been: Wellness programs at news companies I worked for always seemed pointless, and I never signed up.
A painstakingly researched article in the Harvard Business Review explains why corporate well-being programs are failing, and suggests a better way. The overarching theme is simple: Employee wellness programs focus on individual interventions rather than workplace stress. It’s the workplace systems, of course, that make workers unhappy and can squeeze their mental health.
The article breaks down all the reasons that wellness programs don’t work. First, the authors identify five reasons that individual-focused approaches fall short: 1) Employee wellness programs overlook root causes. For example, an employee who badly needs help with excessive stress due to a demanding workload not only won’t get it from a company-sponsored mindfulness app, but will end up feeling hopeless rather than supported when his or her stress level does not improve because the workload didn’t change. 2) They’re seen as hypocritical for just that reason, leading to frustration, annoyance, and a feeling of being pressured. 3) They’re not widely used: Employee Assistance Programs have engaged only about 5-10% of workers since they were developed in the 1980s. 4) They aren’t effective, according to research involving tens of thousands of workers at hundreds of organizations with a range of individual well-being interventions. 5) They lack employer buy-in, with low leadership engagement in promoting or tracking outcomes over time.
The article then offers evidence-based solutions which, given the publication, include a return on investment point of view. The authors suggest a “holistic approach” involving broader interventions that they admit can sometimes present implementation challenges or require more significant changes like reimagining workflow or operations that can be a tough sell in the C-suite. But “to truly combat rising need and mitigate the costs of poor well-being, we believe that systemic change is essential,” they write. Their recommended strategies:
1) Respond to employee needs with organizational change, especially addressing workers’ top priority of work life balance and flexibility; four-day work weeks, for example, can return important time to workers, help them manage stress and improve productivity during the hours they’re at work. 2) Support structural changes with clear goals and metrics that might be measured, according to one “gold standard” approach cited in recent research, with a simple four-question well-being module that regularly measures job satisfaction, sense of purpose, happiness and stress levels. 3) Develop grassroots “employee well-being champion networks” with volunteers acting as mental health advocates for their team and delivering feedback and suggestions for improvement to decision-makers. 4) Equip leaders to support organizational change by, for instance, embedding mental health training into their management curriculum. 5) Build accountability.
“By acting as behavioral architects,” the authors write, leaders “can foster a culture that prioritizes mental health and well-being at every level, ensuring that support is deeply integrated into the organization. This approach has the potential not only to enhance employee satisfaction and engagement but also to deliver a strong return on investment on corporate well-being initiatives.”
Lack of attention to workplace mental health in Africa may be costly
Mental health is a low priority in most of Africa, largely due to poorly funded and underdeveloped public health systems and high stigma throughout the continent. The economic consequences are staggering, reports DW (Deutsche Welle), a publicly funded German news organization that covers the world and broadcasts in 32 languages. Businesses don’t prioritize or support their employees’ mental health needs.
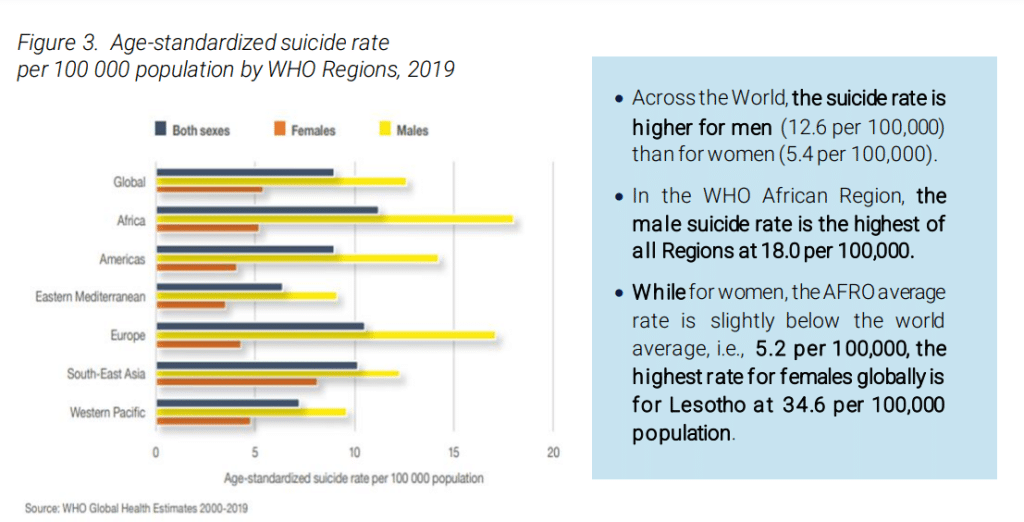
Africa has the highest suicide rate of any global region, according to a World Health Organization fact sheet titled Suicide in Africa, a neglected reality – 11.2 per 100,000 population, in 2019, likely a significant underestimate, compared with a global average of 9.0. (The U.S. suicide rate was 14.5 per 100,00 in 2019, according to the WHO.) More than 75% of suicide deaths on the continent were in low- and middle-income countries. Lesotho, Eswatini, Zimbabwe, South Africa, Mozambique, Central African Republic, Botswana, Eritrea, Cameroon, and Ivory Coast had among the highest suicide rates in the world, topping out with Lesotho’s 87.5 per 100,000.
Uncertainty, poverty, and insecurity are huge issues around the world, as is burnout in workplaces. An estimated 12 billion working days are lost every year to depression and anxiety, at a cost of $1 trillion annually in lost productivity, according to the WHO. In Africa, workplace mental health is largely overlooked despite the likelihood that high stress is leading some employees to quit. “As HR, we need to plan the workforce properly,” said Cynthia Kodowu, a Ghanaian human resources specialist “We’ve created a culture where people feel obliged to take on more just to prove themselves. We’re trained not to complain. We’re trained just to say it’s OK, give it to God, you’re going to get better.”
But at least one African country has low-cost alternatives to regular therapy in Africa, such as grandmother benches and friendship benches, developed by Zimbabwe psychiatrist Dixon Chabanda. In this model, grandmothers trained as lay therapists take turns sitting on benches and being available to talk with villagers or townspeople suffering from depression, anxiety and other mental health problems. It’s a movement that has helped the world re-imagine mental health care: One African study has shown the popular model to be more effective than regular therapy, and the model is going global, as MindSite News noted last year.
News roundup: Striking findings on a new (potential) addiction treatment, Narcan success rates, and more
Could Ozempic be a breakthrough drug for addiction, too? A new class of medications like Wegovy, Ozempic, and Mounjaro that that are proving effective in treating obesity and diabetes – and exploded into Americans’ consciousness as off-label weight-loss drugs, causing shortages for those who really need them – might also help fight the nation’s most intractable drug problems, writes Maia Szalavitz, the New York Times opinion section’s resident expert on addiction.
Now, eye-opening data from two studies of what are known as GLP-1 receptor agonists provide promising evidence for that possibility. A study published last Thursday in Addiction examined the medical records of over a half-million people with opioid use disorder and found that those who were taking GLP-1 medications for any reason had a 40% lower overdose risk than those who were not. The study also looked at the medical records of 800,000 people with a history of alcohol use disorder, finding that the number of doctor visits that noted current alcohol intoxication was halved in patients who were prescribed the drugs compared with those who were not.
Another large study of people with both opioid use disorder and Type 2 diabetes that was published in JAMA Psychiatry two months ago found that the risk of being hospitalized for overdose was reduced by 40% to 70% in patients who took semaglutide (sold as Ozempic or Wegovy) rather than older diabetes medications.
These kinds of studies can’t prove that the drugs can treat addiction. But if more rigorous studies find similar benefits – early clinical trial data is promising – the GLP-1 medications could turn out to be as big a breakthrough for addiction treatment as they have been for obesity. Scientists still need to figure out how they drugs work.
For anti-addiction medications, the ideal outcome would be increasing satisfaction with what users consume, without creating disgust or limiting their ability to experience pleasure. None of the three medications approved to treat addiction – methadone, buprenorphine, and extended-release naltrexone – even attempt to do that.
Methadone’s moment? Methadone is the longest-used and most studied treatment for opioid addiction, and generally the most effective for hard-core users living on the street. A study in JAMA that looked at the medical records of 31,000 Canadians treated for opioid use disorder (OUD) found that people, particularly fentanyl users, were more likely to stay in treatment if they received methadone compared with Suboxone (a combination of buprenorphine and naloxone), the Politico Future Pulse newsletter reported.
The numbers don’t seem that different, or good: 88.8% of people prescribed Suboxone stopped treatment within two years compared with 81.5% of those on methadone. But the adjusted hazard ratio was 1.58, indicating a 58% lower chance of stopping treatment on methadone compared with Suboxone. Mortality risk during OUD treatment with either drug was similar. Both medications were available through doctors’ offices and specialized drug treatment centers in British Columbia. South of the border, methadone can only be prescribed and dispensed in opioid treatment programs (OTPs), aka methadone clinics.
A combination of recent federal policy advances and the Modernizing Opioid Treatment Access Act, a bipartisan bill that is awaiting congressional approval, “could catalyze a sea change in OUD care delivery, matching the unprecedented health crisis that our nation faces,” three researchers wrote in a JAMA commentary headlined “Methadone’s Moment.” The bill would allow physicians unaffiliated with methadone clinics to prescribe the medication and is supported by many experts and multiple medical organizations, including the American Society of Addiction Medicine. It has broad support in the upper chamber but faces a steep uphill battle in the House. “Its enactment remains uncertain amid policymaker apprehension and fierce opposition from [opioid treatment programs] trade groups and private equity firms who have invested in OTPs,” the commentary’s authors wrote.
Bystanders’ use of overdose antidote spikes: Administering naloxone − the emergency opioid overdose reversal medication available to consumers as the Narcan nasal spray – increased more than 40% from June 2020 to June 2022, according to findings of a study in JAMA Network Open. There have been increasing efforts in recent years to make naloxone more widely available, and the Biden administration last spring announced plans for “flooding the zone” with the lifesaving medication.
The findings show that “public health efforts are working,” Chris Gage, lead author of the study and EMS research fellow with the National Registry of Emergency Medical Technicians, told CNN. “There’s no real medical training required,” Gage said. “It’s pretty much as easy as spraying Afrin up someone’s nose. Just showing people that they could do something to potentially save someone’s life is the ultimate goal.”
Data from the National Emergency Medical Services System showed that 744,078 patients received naloxone during EMS activations over the two-year study period, in some cases before the crew arrived. Naloxone administration overall declined 6.1% over the two years while administration by laypeople increased 43.5%. Still, that represented just 24,990 patients, or 3.4% of the total.
The decades-long trend of fast-increasing overdose deaths reversed over the last year or so, with the most recent CDC provisional data showing a 12.7% drop for the 12 months ending May 2024 compared with the same period a year earler – a big difference from the earlier study period, when overdose deaths climbed by nearly a quarter over the two years.
Narcan, which is distributed for free by opioid treatment programs, syringe exchanges, advocacy groups and the government, has only gradually become available in pharmacies with the FDA approving an over-the-counter nasal spray version last year. But it typically costs between $40 and $50 for a two-dose package, depending on the retailer. That’s a major impediment for people who want to buy Narcan in case they spot a drug-using neighbor or someone on the street barely breathing, often indicating an overdose.
In other news…
More than 2,400 mental health workers at Kaiser Permanente went on strike Monday in Southern California, CalMatters reported. They want more time between appointments to prepare for patients, as well as a wage increase and pension benefit that the company provided to its Northern California clinicians as a result of a 10-week strike two years ago that led Kaiser to commit to hiring more therapists give employees specific work hours away from face-to-face patient care.
On Monday morning, mental health employees represented by the National Union of Healthcare Workers established picket lines at locations from Los Angeles to San Diego. Kaiser said in a statement that it was notifying clients whose appointments could be affected by the strike. “Patients will have the opportunity to be seen by another professional in our extensive network of highly qualified, licensed therapists, if their regular provider is engaged in a strike,” the statement said.
If you or someone you know is in crisis or experiencing suicidal thoughts, call or text 988 to reach the 988 Suicide & Crisis Lifeline and connect in English or Spanish. If you’re a veteran press 1. If you’re deaf or hard of hearing dial 711, then 988. Services are free and available 24/7.
Recent MindSite News Stories
In Chicago, Immigrants Who Fled Violence and War Struggle With Their Mental Health
Many immigrants suffer from trauma as a result of the persecution they fled and their perilous journey to the states. The city of Chicago is trying to help meet those needs. Continue reading…
Avoiding distracted driving is a bigger challenge for people with ADHD
Getting distracted, impulsivity, poor judgment and thrill-seeking tend to appear more often in drvers with the disorder. Continue reading…
Driving with ADD: Medication was the answer for one teen driver

Teen driver Hannah Henderson, who has attention deficit disorder, says medication helped her focus on the road. Continue reading…
If you’re not subscribed to MindSite News Daily, click here to sign up.
Support our mission to report on the workings and failings of the
mental health system in America and create a sense of national urgency to transform it.
For more frequent updates, follow us on Facebook, Twitter and Instagram:
The name “MindSite News” is used with the express permission of Mindsight Institute, an educational organization offering online learning and in-person workshops in the field of mental health and wellbeing. MindSite News and Mindsight Institute are separate, unaffiliated entities that are aligned in making science accessible and promoting mental health globally.
Copyright © 2021 MindSite News, All rights reserved.
You are receiving this email because you signed up at our website. Thank you for reading MindSite News.
mindsitenews.org
The name “MindSite News” is used with the express permission of Mindsight Institute, an educational organization offering online learning and in-person workshops in the field of mental health and wellbeing. MindSite News and Mindsight Institute are separate, unaffiliated entities that are aligned in making science accessible and promoting mental health globally.


Author



