Baby Talk Directed at Elders ‘Doesn’t Feel Good’
Using “elderspeak” makes older people feel like babies. And in California, some police departments won’t respond to mental health calls.


Tuesday, May 20, 2025
Good Tuesday morning!
Here’s the Daily lineup: “Elderspeak” makes older people feel like babies. In California, some police departments are refusing to respond to mental health calls, raising lots of questions.
Plus: Quitting benzos can be torture. How can you tell if online health content is trustworthy? Elderly people reap significant benefits from stopping antipsychotics prescribed during hospital stays. And more.
But first: After years of lefty associations, psychedelics are in vogue with the American right. A guest essay in the New York Times explains how that happened. (Hint: billionaires.)
‘Sweetie, are we ready to take our bath?’: Infantalizing through elderspeak
Carol Fahy’s mother is blind, in her 80s, and lives in an assisted living facility near Cleveland. Staff there call her sweetie and honey babe; they also “hover and coo, and they put her hair up in two pigtails on top of her head, like you would with a toddler,” said Fahy, a psychologist in Hawaii. “It doesn’t make someone feel good,” she told the New York Times.
It’s also classic “elderspeak”: talking to an older person in the same, soft tones you might use for a child. It might include terms like dearie, or plural pronouns — Are we ready to take our bath? — or use a singsong vocal quality, along with words like potty or jammies. Elderspeak, however well-intentioned, “arises from an ageist assumption of frailty, incompetence and dependence,” said Clarissa Shaw, a dementia care researcher at the University of Iowa College of Nursing. She evaluated videotaped interactions between nursing home staff and residents with dementia and found that 84% of the transcripts included at least one example of elderspeak. Other studies have found a relationship between elderspeak and nursing home residents adopting resistant behaviors like clenching their mouths shut when health aides try to feed them.
In an effort to reduce elderspeak, Shaw and her colleagues developed a training program called CHAT (for Changing Talk) that uses videos of communication between staff and patients. They tested it in 13 nursing homes and found that elderspeak went from being used 35% of the time to 20%. In another study, CHAT training was associated with lower use of antipsychotic drugs. The team is now streamlining and adapting the CHAT training for online use, and studying its impact in around 200 nursing homes nationwide.
The example of elderspeak that bugged me the most wasn’t even in a nursing home. After Lisa Greim, 65, a retired writer in Arvada, Colo., enrolled in a Medicare prescription drug plan, a mail-order pharmacy began calling almost daily because she hadn’t filled a prescription. These “gently condescending” callers, apparently reading from a script, all said It’s hard to remember to take our meds, isn’t it? – as if they were all swallowing pills with her. Annoyed, she asked them to stop calling. (They did.)
Some California police are no longer responding to mental health calls – so who should be?
In a newsletter item last month, my colleague Courtney Wise covered the move by Jim Cooper, the sheriff of Sacramento County in California, to no longer respond to mental health calls that don’t involve a threat to someone’s life or a crime. The item was based on an in-depth piece for CalMatters by Lee Romney, a contributor to MindSite News and former LA Times reporter, who told the story of families affected by the policy, and dug into the factors influencing the change. She reported that counties like Sacramento and Orange want to get “out of social work,“ as Orange County Sheriff Don Barnes put it.
Cooper had been pondering a pullback for a year, pushed by his conviction that officers are not trained mental health professionals and by a federal appeals court ruling that he believes heightens his officers’ liability in non-criminal mental health calls. The law firm that advises state police chiefs and sheriffs associations disagrees with Cooper’s legal assessment, as do others. But the Del Norte County Sheriff and Crescent City Police Department have recently adopted similar policies.
The issues, as Romney pointed out, are longstanding and thorny: “Because mental illness isn’t a crime, when should law enforcement be involved, if at all? Who is best suited to safely de-escalate a mental health crisis and coax a person to accept care? And what if that person won’t – or due to the nature of their psychosis or substance use cannot – agree to go voluntarily? Who will transport them for involuntary psychiatric holds?”
Our friends at the health policy podcast Tradeoffs also picked up on Romney’s story, and interviewed her for a recent podcast. She described a recent case in Sacramento where the sheriff’s department declined to respond to a 911 call involving a young woman who was threatening her mother and step-father with a knife while they were locked in their bedroom. A supervisor, implementing the new policy, said they would not send officers to the scene and expressed hope that the daughter would calm down.
Romney made two especially interesting points: One was that in this case, emergency dispatchers at 911 did not attempt to transfer the call to 988, the suicide and crisis lifeline. “They just said, ‘Stay in your locked bedroom,'” Romney noted. But, she told Tradeoffs, the policy has “accelerated the effort to integrate 911 and 988 so that they can actually do like a direct warm handoff when someone calls 911 to 988. That was not happening before the policy shift… (Now) they’re getting the word out about 988.”
Since more than 2,000 people experiencing a mental health crisis have been killed by police over the past decade, this policy shift is being cheered by some peer advocates whose experience with police response has left them deeply skeptical about the role of police in such incidents. MindSite News has documented many of these cases in our ongoing series, Fateful Encounters, including this story, published last week.

Social Worker or AR-15? Portland Struggles Over How to Respond to People in Mental Health Crisis
By Audrey Azzo • Investigations • May 12, 2025
The torment of quitting benzos
Benzodiazepines like Xanax, Ativan and Valium, are good at what they do – treating anxiety, panic attacks and insomnia – and are familiar to many, with 92 million prescriptions dispensed in the United States in 2019. Though they don’t cause many overdose deaths on their own, they frequently are used in combination with opioids, and they have a lot in common: Both can create physical dependence in weeks, and quitting requires a gradual tapering to avoid withdrawal symptoms, something prescribing doctors aren’t always experienced with. As a result, they can be reluctant to write prescriptions for both types of drug, making it hard for patients with a legitimate prescription to avoid painful periods of withdrawal.
“Benzos generate as much anxiety in the prescriber as they do in the patient,” Ronald M. Winchel, a Columbia University psychiatrist, told the New York Times. “Do I start it? … Is it safe? Is my patient going to abuse it? What will my colleagues think?” (Prescriptions have been declining since 2016, partly because of these concerns.)
Even though benzodiazepines have been around since the 1960s, physicians are often unaware of how to best help their patients stop taking these drugs, in part because there is no one-size-fits-all tapering strategy. To address those issues, the American Society of Addiction Medicine two months ago released detailed clinical guidance on tapering. They recommend that clinicians assess the risks and benefits of ongoing benzodiazepine prescribing at least every three months, and, when tapering, consider reducing the current dose by 5 to 10 percent every two to four weeks. Patients who have been taking benzodiazepines for years may require more than a year of tapering, and should be monitored even after the drug has been discontinued. A sudden stoppage is not advised.
Tasha Hedges took Xanax for 20 years to treat anxiety and panic attacks, under a psychiatrist’s guidance. In 2022, that doctor died. When she eventually found a new psychiatrist, “the first thing he did was start yelling at me that I had been on Xanax too long,” said Hedges, 41. “He ripped me off my meds.” Her experience quitting cold turkey was “a nightmare“ of hot flashes, cold sweats, restless legs, the shakes and teeth grinding. She’s still dealing with the fallout, two years later: “My brain has not been the same.”
The Medicaid dilemma dividing House Republicans: How massive – and catastrophic – should their cuts be?
As the sun set on Monday, the extent of proposed Medicaid cuts – severe vs. more severe – still sharply divided House Republicans, with many hoping that President Donald Trump will be able to close the gap when he joins the debate at a party meeting Tuesday morning, Reuters reports. GOP leadership hopes Trump can convince hard-liners to forego deeper cuts, according to Politico.
Trump has supported Medicaid-cutting schemes, despite his previous insistence that the program would not be touched. The current impasse pits a handful of hard-right members, who lost a fight to make major structural changes to the program but insist on greater cuts, against those who want less extreme cuts.
A key committee approved the bill’s latest iteration late Sunday, but only because its most conservative members voted “present,” leaving the hard choices for debate on the floor.
Last week, the Congressional Budget Office estimated that proposals to impose work requirements on people enrolled in Medicaid starting in 2029 would cause 8.6 million people to lose coverage. Since then, new proposals would start the work requirements even sooner and save more money, Politico reports.
- The BBC described the major sticking points as of Monday.
- A Health Affairs Forefront piece (published last Wednesday) analyzes all the major health-coverage provisions in the Republican legislation in greater detail.
- And a New York Times opinion piece explains why the Medicaid work requirements are cruel – and, crucially – pointless.
In other news…
Tips for ferreting out trustworthy health content online, courtesy of a Psychology Affairs blog post by Shannon Sauer-Zavala, a licensed clinical psychologist and associate professor of psychology at the University of Kentucky. She advises asking three core questions about information viewed on social media:
- Credentials: Do information providers have training, licensure, or clear professional experience?
- Transparency: Are they clear about what they’re offering (and selling)?
- Nuance: Do they acknowledge complexity – or just promise five-step fixes?
- Accountability: Are they referencing actual research or clinical best practices?
What happens when elderly patients come off hospital-prescribed antipsychotics? Good things! There’s been a long push to reduce prescribing of antipsychotics in nursing homes, where they are frequently and inappropriately used to manage behavioral disturbances in elders. Less attention has been paid to their use among the same population and for the same reasons during hospital stays.
Now a new study has tracked what happened to some 27,000 older patients who were prescribed antipsychotics in the hospital and then discharged. Some – “continuers” – stayed on the meds after leaving the hospital; others – the “discontinuers” – did not. During six months of follow-up, the “discontinuers” had significantly lower rates of just about every metric studied including rehospitalization, inpatient delirium, fall-related emergency department visits, urinary tract infections leading to hospital stays, and death from any cause.
The findings, researchers wrote in JAMA Psychiatry, suggest that antipsychotic medications should be taken “for the shortest possible duration“ and “discontinued in a timely manner.”
The name “MindSite News” is used with the express permission of Mindsight Institute, an educational organization offering online learning and in-person workshops in the field of mental health and wellbeing. MindSite News and Mindsight Institute are separate, unaffiliated entities that are aligned in making science accessible and promoting mental health globally.


Author

Related Articles
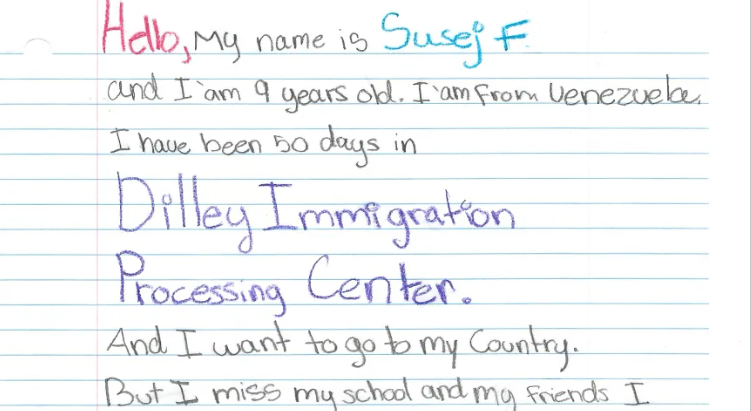
Health Organizations Condemn Traumatic ICE Raids, Family Separation
According to letters from children living in an ICE detention facility, living conditions are inhumane and their mental health is suffering.

In Teens, Social Anxiety Often Looks Like Anger
A study finds that some teens’ aggressive behavior may be due to social anxiety, not straightforward reactivity.

Expert Calls for Harm Reduction, Not Punishment, to Resolve Our Overdose Crisis
As the Trump administration pulls funding from harm reduction, an expert on the overdose crisis says it’s the best way to save lives.