NAMI Director Explains New Laws to Keep People with Mental Illness out of Jail
The National Alliance on Mental Illness (NAMI) is advocating for state laws to divert people with mental illness from jail and into treatment, highlighting Florida’s Tristin Murphy Act as a national model.

With an estimated 1.2 million people with serious mental illness locked up in the nation’s prison and jails, advocates continue to push for more options to divert people to care instead of incarceration.
This month, the National Alliance on Mental Illness (NAMI) issued a report calling for states to do more to keep people with mental illness out of prison and to invest more in caring for the mental health needs of those who are already there. The report singled out the Tristin Murphy Act, a 2025 Florida law named after a man who died by suicide in a Florida prison.
The law strengthens diversion policies in Florida by expanding grants to train 911 operators and emergency medical technicians on crisis intervention. It also allows jails to screen people charged with a crime for mental illness 24 hours after being booked and provide alternative options to incarceration, according to the brief.
“We hope to bring light to the tragedies that result from the overincarceration of people with mental illness,” Stephanie Pasternak, director of state affairs at NAMI, told MindSite News in an email. “We also want people to understand that this problem is preventable with the right diversion policies, which can help people get connected to the care they need.”
The report highlights the large numbers of people with mental illness who are incarcerated — 40% of people in jail or prison have a history of mental illness. It also points to legislation in Oklahoma, Nebraska, Washington, Minnesota, Colorado, Texas and Oregon as further examples of ways to keep people with mental illness out of jails.
The legislation broadly focused on six categories: diversion, juvenile justice, conditions in custody, re-entry, competency restoration and civil commitment.
“State lawmakers and advocates can use this brief to identify promising laws from other states that they want to replicate to help reduce the criminalization of mental illness,” said Pasternak.
MindSite News interviewed Pasternak to learn more about NAMI’s recommendations. The interview has been edited for brevity and clarity.
Josh McGhee: Why did you choose to highlight Florida?
Stephanie Pasternak: Tristin Murphy died by suicide in a Florida jail in 2021 after the jail failed to identify and treat his mental illness. NAMI advocates often work to bring the lived experience stories of peers and family members before policymakers. In this case, NAMI advocates in Florida worked with Tristin Murphy’s family and other advocacy groups to bring Tristin’s story to the attention of the Florida legislature, governor’s office, and local media. (Editor’s note: CBS Miami produced a documentary, Warehoused: The Life and Death of Tristin Murphy).
Jail suicide is a national issue – suicide is the leading cause of death for people who are incarcerated in jails, accounting for about 30% of all jail deaths. The Tristin Murphy Act (SB 168) enhances mental health screening in jails. It also allows for people being held for non-violent offenses to be eligible for mental health diversion programs that can connect them to treatment and help them avoid incarceration.
The reality is that many people with mental illness who are incarcerated are held for committing non-violent, minor offenses related to the symptoms of untreated illness (for example, disorderly conduct, loitering, trespassing, disturbing the peace) or for offenses like shoplifting and petty theft. Incarcerating people for these low-level crimes is not only counterproductive and harmful to the individuals and families, it’s also extremely expensive for state governments.
Current data tells us that at least 27 states have pre-trial diversion. But even for states with pre-trial diversion, these programs can and should be strengthened.
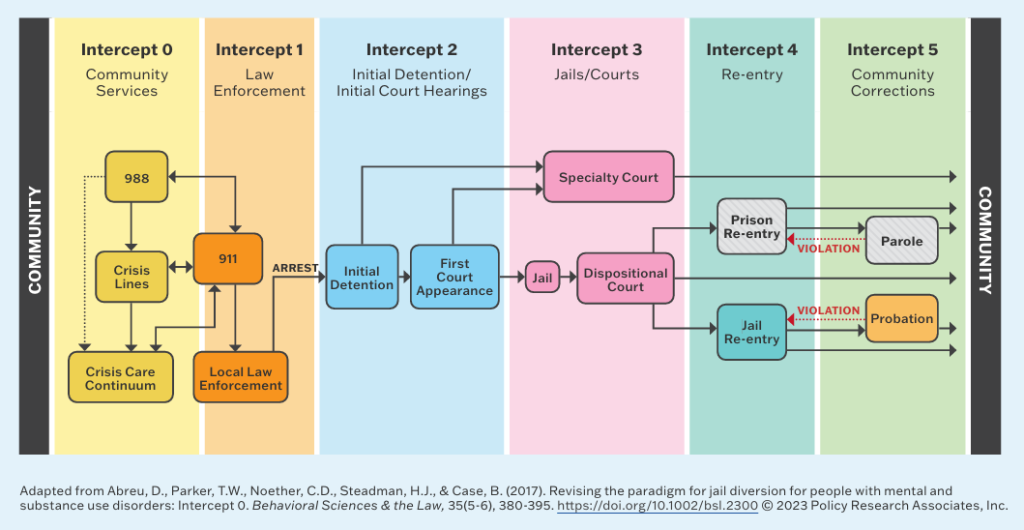
You talk a lot in the report about the “Sequential Intercept Model” – can you explain it and why it’s important?
The Sequential Intercept Model (SIM) is an evidence-informed tool that helps communities identify opportunities and needed resources to help divert people with mental illness away from the justice system and into mental health care.
SIM includes five intercepts, ranging from Intercept 0 (which refers to community services aimed at preventing any criminal justice system involvement) to key intercept points along the criminal justice system continuum (including law enforcement contact, initial arrest/detention, jail and courts, reentry, and community corrections).
We’ve put a heavy focus on this model because it’s a helpful way for policymakers to understand where they can make a difference with the legislation they introduce. States should have policies in place that address diversion at every intercept.
Wouldn’t it be most beneficial to focus on expanding early intervention or improving things at the first intercept, before involvement with law enforcement?
NAMI strongly believes that the best solution for diverting individuals with mental illness away from criminal justice system involvement is through early intervention, comprehensive community mental health care, and a robust crisis response system.
NAMI wants everyone to be served at Intercept 0, before they have any justice system contact. However, we cannot ignore the fact that many people don’t receive a diagnosis or have access to care until they come into contact with the criminal justice system. Even as mental health services grow, our mental health system is far from perfect and law enforcement regularly encounters people with mental illness.
This reality means we need to have the right policies in place to make sure that any contact with law enforcement or the justice system leads to people gaining access to care and not being trapped in a cycle of incarceration.
This issue brief is the first of three that NAMI will be publishing this year. In May and July, we will be focusing on more upstream approaches with issue briefs dedicated to access to care and 988 and crisis response respectively.
What do you say to communities that are hesitant to involve police in their models of care?
There can be hesitancy to involve police in planning for mental health crisis response, and that is understandable when police involvement has sometimes led to tragic consequences. While it is important to reduce the role of law enforcement in mental health crisis response, they are currently the primary responders to mental health crises in most communities. Their knowledge of local systems, services, and trends can be essential to identifying gaps and opportunities.
In addition, there also may be instances where law enforcement will need to be part of a crisis response, so getting their buy-in early is helpful.
People with severe mental illness are often deemed by courts to not be competent to go to trial or assist in their own defense and end up languishing in jails waiting for mental health assistance to “restore competency.” What are your recommendations about this?
One of the biggest problems with competency restoration services is that they are designed to make sure people can understand the criminal charges against them and can participate in their own defense, rather than actually treating their underlying mental illness. Because of this, even when individuals are restored to competency, we see them cycle back into jail because they still haven’t received adequate mental health treatment.
This is one reason why NAMI is in favor of community-based competency restoration, delivered by community mental health treatment providers. By connecting someone to care in the community, providers can address both competency and long-term recovery. This sets someone on a path to stay engaged in their care and can eliminate disruptions to care when someone moves from the justice system back into the community. The sooner we can connect people to consistent services in the community, the greater chance they have of staying engaged in long-term recovery.
MindSite News has reported on people being involuntarily committed when they didn’t believe they were a danger to anyone or in a mental health crisis. How do we ensure laws that expand commitment standards aren’t abused by family or law enforcement?
The civil commitment system is broken. Laws that are written too narrowly mean that far too many people fall through the cracks and end up in a cycle of homelessness or incarceration. Laws that are written too broadly risk people having their civil rights unnecessarily trampled. At NAMI, we advocate for a balanced approach to reforms — protecting individuals’ rights but also allowing the system to intervene when necessary.
Having policies that enforce strong due process protection is critical. Laws should be clear about what qualifies someone for commitment, who can initiate proceedings, timeframes for initial commitment and court proceedings, access to legal counsel, right to multiple and independent evaluations, and regular redeterminations hearings — all are measures that can help protect commitment laws from being abused.
Courts and mental health systems need to work together as close partners to ensure commitment is only being used when clinically necessary and that someone’s individual rights are not being ignored.
The name “MindSite News” is used with the express permission of Mindsight Institute, an educational organization offering online learning and in-person workshops in the field of mental health and wellbeing. MindSite News and Mindsight Institute are separate, unaffiliated entities that are aligned in making science accessible and promoting mental health globally.
Author

Related Articles

Can ChatGPT Be Your Therapist? This Therapist Found Out for Herself
Can ChatGPT offer a viable alternative to traditional therapy? In this first-person essay, a licensed therapist explores that question.

What Was I Made For? Identity, Meaning, and the Emotional Cost of AI
Machines can now write, analyze, diagnose, and simulate emotional presence, triggering not just a technological disruption but one that strikes at who we think we are.

Brown University Shooting Again Reveals Why Trauma Care Must Begin Before People Seek It
A former Brown student and longtime mental health journalist says that how institutions respond after traumatic events can shape mental health outcomes for years to come.