Research Roundup: The Predictive Power of the Brain
The antidepressant fluvoxamine (Luvox) appears to be effective for Covid-19, reminding us that the term “antidepressant” may not fully describe this medication.

This Week in Mental Health Research
Hello readers. It’s been a busy week with Halloween, Dia de Los Muertos, Diwali, plus elections in many places. So you can be forgiven for missing some important stories from the world of mental health research. Did you know that investments in family benefits correlate with rates of child maltreatment? Or that an inexpensive antidepressant may be one of the best current anti-Covid medications? Read on, to make sure you don’t miss out on the latest from the world of mental health research. This column does not claim to be comprehensive nor does it promote the science cited. It will appear on the MindSite News website and will be sent to subscribers of our Research Roundup newsletter. You can sign up for our newsletters here.
By Tom Insel, MD
State Benefits Matter for Child Maltreatment
Child maltreatment is a profound public health problem in this country. In 2018, 3.5 million children were part of a child abuse investigation, 768,000 were substantiated as victims, 207,000 received foster care services, and 1,770 died of abuse. These kinds of numbers should inform the ongoing debate about federal support for families and children – as well as debates about state investment, since states differ greatly in how they support families and in rates of reported maltreatment.
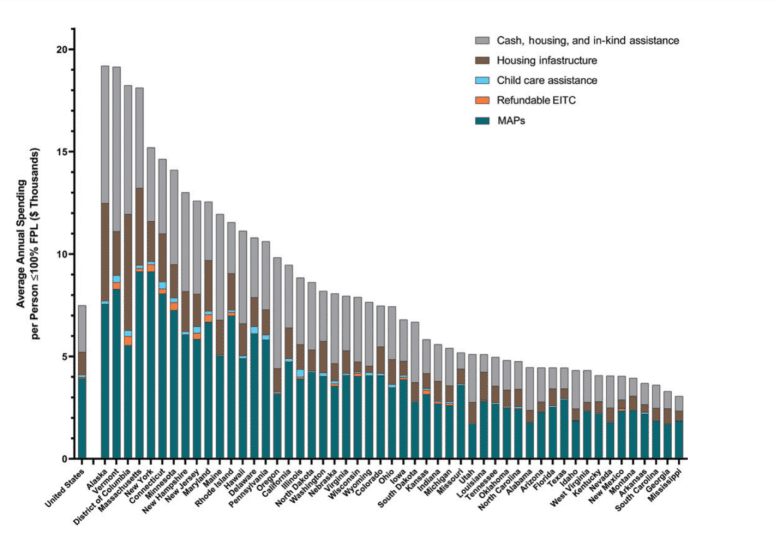
In a new report in the journal Pediatrics, Henry Puls and colleagues explore the relationship between state spending on benefits programs – including cash, housing and childcare assistance, earned income tax credits and medical assistance like Medicaid and CHIP – and rates of maltreatment. The outcomes measured were reports to child-protective services, substantiations of harm, foster care placements, and ultimately, deaths of children – more than 12,000 kids died of abuse during the eight study years.
Puls and his team found great variation in benefits among the 50 states and a strong link to rates of maltreatment. Across the states, every one of the maltreatment variables was associated with state investment in benefit programs. In fact, for every additional $1000 spent for each person living in poverty, reports of maltreatment rate fell 4.3%, substantiated reports dropped 4.0%, foster care placements dropped 2.1%, and child deaths fell 7.7%.
A comparative international study published last year had a blunt message: “The richest country in the world, the USA, has the highest rates of child abuse and total child mortality in the Western world.”
The numbers in this new study suggest that a 13.3% increase in state spending on benefit programs – at the cost of $46.5B nationally – might lead to 28,500 fewer cases of substantiated child maltreatment, 4,100 fewer children requiring foster care, and 130 fewer children dying from abuse.
As Congress and state legislatures debate spending levels for social programs, data like this should be understood and considered.
State Spending on Public Benefit Programs and Child Maltreatment Pediatrics, Oct 18, 2021
Can the Brains of People Who Undergo Trauma Predict How Well They’ll Cope?
People who live through traumatic events like a car crash, combat or violence experience a range of reactions. While almost everyone has a short-lived “acute stress response,” a few go on to have ongoing, chronic problems including distressed sleep, intrusive thoughts or dreams and panicked reactions for months and years after the trauma — the condition we famously call post-traumatic stress disorder or PTSD. How can we predict who will recover and who will struggle with PTSD? That’s the central question of a longitudinal study called AURORA that has been tracking the mental health outcomes of people treated for trauma in 22 emergency departments across the country. Before this study it was clear that symptoms of distress in the immediate aftermath of a trauma didn’t predict longer-term outcomes. Nor was there a simple blood test or cognitive assessment that could distinguish who would recover and who would progress to PTSD.
Now, in one of the first reports from the AURORA project, a team led by Jennifer Stevens of Emory University used a type of brain imaging called fMRI to peer into the brains of people two weeks after the traumatic event. Stevens’ teams exposed the patients to different potential triggers – fearful vs. neutral faces, the prospect of monetary gain or loss, and a simple test of vigilance. Using fMRI is not practical in routine practice because the technique relies on group differences that are not useful for individual clinical decisions. But while the AURORA project is not a guide for clinical care, this ambitious study does deserve note.
In the first 69 volunteers, all victims of car collisions, four patterns of response were seen, and were mostly replicated in an independent sample. In both samples, one subgroup – whose brains most actively responded to both threat and reward – was the most likely to continue having PTSD symptoms at six months.
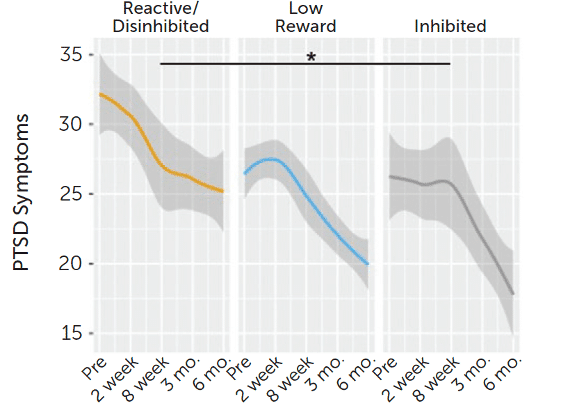
This finding suggests that brain biotypes could be used for identifying subgroups that can’t be discerned by clinical examination. If we could identify that fraction of victims at highest risk for PTSD, prevention efforts could be targeted to have the biggest public health impact. Yet the AURORA findings, while statistically significant, don’t provide a path to action since they are conflated by many things: life before and after the traumatic event and the nature of the trauma itself.
Samuel Johnson famously noted, “How small, of all that human hearts endure, that part which laws or kings can cause or cure.” The same might be said for prediction. Even for a project as ambitious as AURORA, predicting – and altering – the fate of an individual trauma victim may be beyond our current approaches.
Brain-Based Biotypes of Psychiatric Vulnerability in the Acute Aftermath of Trauma American Journal of Psychiatry, Oct 14, 2021
A little-used antidepressant’s new potential as an anti-Covid therapy
Nearly every medication has multiple biological effects, some welcome, some not. Aspirin is a pain reliever, a fever reducer and a clot blocker. Sildenafil (Viagra) was developed for pulmonary hypertension. Now, in a surprising star turn, the antidepressant fluvoxamine (Luvox) appears to be effective for Covid-19.
A few reports over the past year suggested that fluvoxamine might reduce the severity of Covid-19 infections so Gilmar Reis and his collaborators across Brazil included it among several currently available, inexpensive medicines repurposed as Covid treatments in a large clinical trial for a population that has had limited access to vaccines.
In the first half of this year, 1500 Covid-infected patients were randomized either to fluvoxamine (100mg twice daily for 10 days) or placebo. In the fluvoxamine group, 11% were hospitalized compared with 16% in the placebo group. Many patients discontinued fluvoxamine after just a few doses, so these results may be difficult to interpret. But for those who took fluvoxamine for the entire 10 days[RW4] , the results were even greater: a 66% reduction in hospitalization. Of that group, there was one death in the fluvoxamine group and 12 deaths in the placebo group. These differences were significant enough that the trial was stopped at an interim point so that fluvoxamine could be used clinically for all.
It’s important to remember that these Covid-positive patients were not diagnosed with depression or any other mental illness. Indeed, the differences between drug and placebo in this study surpass some of the results of drug vs. placebo for the treatment of depression. These effects are also comparable to or better than many of the current anti-Covid treatments being studied, including monoclonal antibodies.
The effects of fluvoxamine on Covid progression are likely due to the drug’s anti-inflammatory properties, although this has yet to be proven. It is also not yet clear if other SSRI antidepressants will be as effective for Covid. But this surprising finding with fluvoxamine reminds us that the term “antidepressant” may not fully describe the pharmacology or the therapeutic potential for this class of medications.
Effect of early treatment with fluvoxamine on risk of emergency care and hospitalization among patients with Covid-19: the TOGETHER randomized, platform clinical trial The Lancet, Oct 27, 2021
Does an Emergency Room Visit for Suicidal Thinking or Attempts Predict Future Suicide?

A critical challenge for preventing suicide is understanding risk. Men are at higher risk than women, older people are at higher risk than younger people, and those with a mental illness or substance use disorder have the highest risk of all. But those risk factors, while substantial, still aren’t enough to predict imminent suicide risk in a medical office or emergency room. A 2019 study estimated that nearly 30% of people who die from suicide had a healthcare visit within seven days and nearly half have been seen in an ER in the previous year. Yet it’s unclear how well an ER visit for suicidal thoughts or even a suicide attempt actually predicts subsequent death from suicide. Indeed, one bit of clinical lore considers people with a history of multiple visits for suicidal thoughts or self-harm as having a low risk for suicide death, perhaps like the boy who cried wolf.
Mark Olfson and his colleagues from Columbia University and the New York State Psychiatric Institute studied suicide mortality in nearly 10 million Medicaid recipients and found that people who made an ER visit for a suicide attempt, suicidal ideation, or other mental health issue had a much greater risk of dying from suicide in the following year than the general population. The numbers were striking: an 18-fold increase for those with a suicide attempt or episode of self-harm, 11-fold increase for those with suicidal ideation, and 3-fold increase for mental health visits without suicidal symptoms. Many of these suicides occurred within 30 days and nearly 75% within 180 days of the ER visit. These people were crying out, but they weren’t crying wolf.
Another important observation: Among those who harmed themselves or attempted suicide, the risk of subsequent death was greatest among those who were diagnosed with a substance use disorder. Among those with suicidal ideation, the highest risk was among the subgroup with an anxiety disorder. And among those with an apparently non-suicidal mental health issue, the highest risk of suicide death was among those diagnosed with a personality disorder, usually borderline personality disorder.
For the emergency room healthcare provider trying to assess risk of suicide, there is rarely certainty. This new study demonstrates that suicide risk is markedly higher following emergency room discharge for people with current or recent suicide attempts or suicidal thoughts. Even for the person who denies current suicidal intent, a history of recent suicidal behavior should raise concern. Suicides can be prevented, especially if we understand who is at highest, imminent risk.
Suicide Risk Among Adults With Mental Health Emergency Department Visits With and Without Suicidal Symptoms Journal of Clinical Psychiatry, Oct 26, 2021
Perceptions of (Dis)Parity
Parity for behavioral health services has been the law of the land since 2009, when the Mental Health Parity and Addiction Equity Act passed by Congress went into effect. The idea was simple: people with health insurance coverage should receive equal access to mental health and medical care. So do consumers – everyday Americans with private health insurance they purchased or obtained from their employer – feel their access to mental health services is, in fact, as good? In a word, no.
Susan Busch of Yale University School of Public Health and Kelly Kyanko of the NYU School of Medicine surveyed privately insured adults who received both mental health and physical health care in the past year. More than twice as many – 21% – felt the mental health services provided by their health plans were inadequate as felt their medical services were inadequate – 10%.
Similar findings have emerged in other reports. A 2019 Milliman report found a five-fold disparity in access to in-network providers for mental health care vs. physical health care.
And a recent McKinsey report, released earlier this year, found that while 71% of employers believe they support the mental health of their frontline employees “well or very well,” just 27% of employees agree.
Recently, the U.S. Department of Labor announced its intention to make parity enforcement a priority. It’s been more than a decade since the Mental Health Parity and Addiction Equity Act was passed by Congress. Recent reports make it clear we are a long way from delivering on the promise of that Act.
Assessment of Perceptions of Mental Health vs Medical Health Plan Networks Among US Adults With Private Insurance JAMA Network Open, Oct 22, 2021
In the US, if you or anyone you know is considering suicide, call the National Suicide Prevention Lifeline at 1-800-273-8255.
Tom Insel, MD, is a psychiatrist, neuroscientist, and former director of the National Institute of Mental Health (NIMH). He is a donor to MindSite News and chair of its Editorial Advisory Board. Dr. Insel’s financial conflict of interest statement, which includes equity and advisory roles in several early-stage mental health technology companies, can be found here.
The name “MindSite News” is used with the express permission of Mindsight Institute, an educational organization offering online learning and in-person workshops in the field of mental health and wellbeing. MindSite News and Mindsight Institute are separate, unaffiliated entities that are aligned in making science accessible and promoting mental health globally.


Authors


Related Articles
Is the ketamine story changing?
Two new reports reveals some unexpected developments in the ketamine story. And a new report shines a light into the lived experience of psychosis.

Thanks for the memories, REM
A new study suggests that recovery from psychosis is more possible than many people think. Another shows that peers might be the best suicide- prevention messengers. And a third shows the role of REM sleep in firming up memories.

Your brain on Covid
A new study suggests that the impact of Covid on the brain may extend beyond our sense of smell. And we examine two studies that examine the impact of race on mental health and services.