CARE Team Expands a Nonviolent Mental Health Crisis Response To All Chicago
The alternative crisis response program will increase staff and vans, but advocates are still pushing for longer hours.

Welcome Back MindSiters,
We’re coming to you a day late after celebrating Memorial Day with our families. In case you missed it, MindSite News’ Chicago Bureau had a big month, picking up two more Peter Lisagor Awards for Best Health Reporting and Best Reporting on Political and Government Reporting.
The two Lisagor awards for the “Policing the Vulnerable” series bring MindSite News to four total Lisagor wins since we launched Diagnosis: Injustice just four years ago. Our first dissected the mental health landscape of Chicago as the nation transitioned the National Suicide Lifeline to the three-digit 988 hotline — topics very much still in the news and ones that we’ll be revisiting today.
In this month’s Diagnosis: Injustice, we get an update from the mayor of Chicago on his plans to continue expanding the city’s alternative crisis response team, which is tasked with handling some of the city’s mental health-related calls. We also talk to the authors of a new study from the University of Chicago Health Lab on the systemic challenges and potential solutions for the nation’s crisis response system — both 911 and 988. Finally, we take a look at the decline in overdoses in Oregon and hear from some experts explaining the good news.
Let’s get into it…
CARE goes citywide – for now. Big Tech wants to kill its funding source

Residents across Chicago – instead of just certain neighborhoods – should now have access to the city’s alternative crisis response team if they find themselves or their neighbors in mental health distress during weekday daytime hours.
Only problem: Mayor Brandon Johnson is counting on revenue from his new social media tax – which technology companies are trying to block in court – to continue operating the program.
On May 13, Mayor Brandon Johnson announced at a press conference that he will use the last of the federal stimulus dollars – $5.2 million allocated during the pandemic – to run the service. Once that is depleted, the program will depend on the mayor’s controversial social media tax, which is estimated to bring in $31 million, to keep the vans roving around the city.
A trade association of giant technology companies including Meta and Google are suing to block the tax, which went into effect on January 1. Many companies are now paying the levies under protest.
“For too long, too many people experiencing trauma and mental illness were met with punishment instead of support,” Johnson said at the press conference at Daley Center Plaza. “With the announcement of our CARE program expansion today, we solidify our commitment to prioritize compassion over criminalization, treatment over trauma, and to meeting our people where they are with the support that they need.”
Last year, MindSite News reported on turmoil within the CARE program that caused a sharp decline in the number of times a CARE team responded to mental health crises.
This left police as the de facto responders to these crises, undercutting the intention of the CARE initiative. Our reporting suggested that there was dysfunction and bureaucratic infighting related to the removal of the police department and fire department from the CARE teams.
Despite the funding and staffing woes, which have hampered alternative crisis teams across the country, Johnson, in a statement to reporters from MindSite News and the Medill Investigative Lab-Chicago, committed to funding and ultimately expanding it.
Prior to the expansion, seven CARE teams — composed of a mental health clinician and an emergency medical technician — were responding to low-risk 911 calls involving mental health issues in specific police districts, mostly on the south and west sides, as well as Uptown, the Loop and several other North Side neighborhoods.
The latest expansion will double the number of alternate response vans to eight, which will be staffed by 20 employees. The city will now be divided into two zones — north and south — with four vans available in each, as outlined in a new program description, with services available on weekdays from 10 a.m. to 4:30 p.m.
“We think this is a huge win in the right direction for Chicagoans,” Any Huamani, an organizer with Treatment Not Trauma, a community-led organization that has pushed to remove police from crisis-response teams and to reopen mental health clinics in Chicago, told MindSite News. But she also vowed to push to expand the program’s hours so it runs 24/7.
“Right now, the hours are very limited. It’s kind of like business hours,” she said. “They don’t work on holidays. They don’t work overnight nor the weekends. And, of course, we know that a mental health crisis doesn’t happen on a schedule.”
Helping 988 and 911 work better together
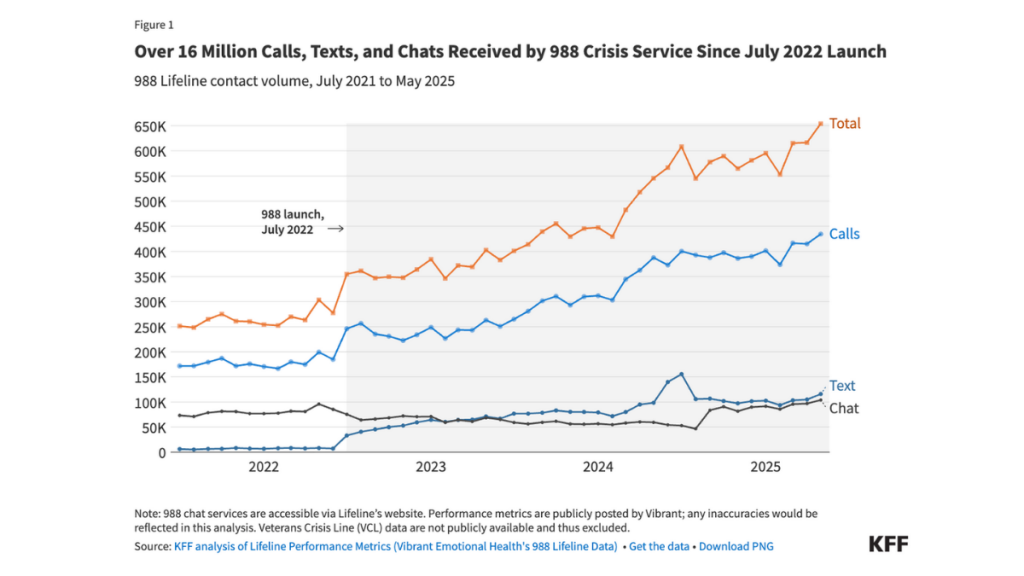
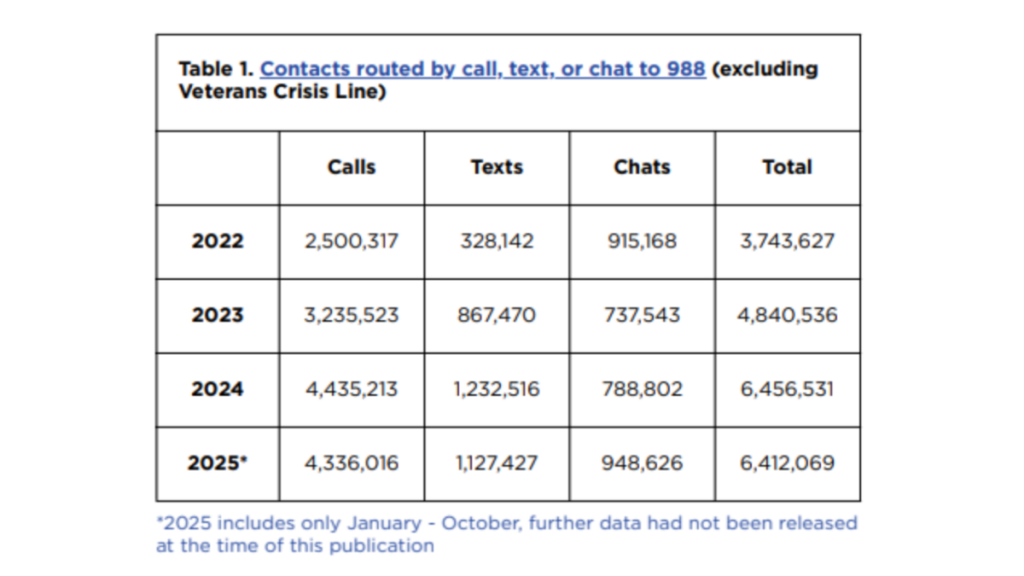
As the 988 Suicide and Crisis Lifeline approaches its fourth anniversary this July, it is in a precarious situation — trying to balance cuts made by the Trump administration to the funding and staff of the federal department that runs it at the same that calls to the hotline continue to grow.
The 988 hotline was created as an alternative to 911 to provide a service for people needing help in a mental health crisis that didn’t require a police response.
Last month, in a new report, experts in crisis response weighed in with their advice on how 988 and 911 can interact better to ensure that no matter which number is dialed, people in crisis get the help they need.
The key is communication, said researchers at the University of Chicago Health Lab, which released the report, “Voices from the Field: A Report on 911 and 988 Interoperability.”
“The 988 and 911 systems and their respective leaders and staff need to be in communication to understand community needs, build trust across hotlines as well as with communities, and provide the best service possible for those in need,” Sarah Scaffidi, senior research manager at the Health Lab, told MindSite News. “Trust is also absolutely critical, and communication goes a long way towards building it.”

The report broke down the problems into three main categories: human, systemic and technological. The authors offer insights and suggestions for improvements based on the experiences of a panel of crisis-response experts they interviewed.
“Despite being a valuable resource, there is a lack of public education about 988 and how it is differentiated from 911 in the minds of many members of the public,” Jessica Gimeno, a mental health policy analyst at Access Living, a Chicago-based nonprofit focused on disability and civil rights, told the researchers. “There is confusion about the distinctions between hotlines: which handle acute crises, which are warm lines and which provide general support. Clarifying these can significantly impact how people seek help and trust these services.”
The experts stress the importance of building trust not just between the two hotlines, but also the communities they are attempting to serve. Many people in different communities including Black, native and LGBTQIA people, don’t trust either 988 or 911 in a crisis.
Advocates for people in crisis are concerned about how people who’ve had prior arrests or are under the influence of drugs will be treated when they call the hotline.
Any trust built in 988 could be wiped away by transferring a call from 988 to 911, especially in those communities with strained relationships with law enforcement, according to the report.
“Trust is deeply rooted in equity,” says Tansy McNulty, founder of 1 Million Madly Motivated Moms, a nonprofit organization focused on eliminating police violence, in the report. “Communities of color have distrust in 911, and that distrust spilled over into 988.”
Adding another challenge, 911 and 988 dispatchers may not trust each other and fear liability if they transfer the call to the other and something bad happens. Staff at 988 are reluctant to transfer calls to 911, fearing an armed response may lead to injury or arrest, the experts said.
Tiffany Patton-Burnside was the senior director of crisis services at the Chicago Department of Public Health in September 2021 when mobile crisis teams began heading out in vans to the scene of mental health emergencies as part of the new CARE program. It took time and effort to build trust between the multiple agencies involved, she said.
“It has taken a long time to indoctrinate our program into the call center, even with the clinicians there every day to facilitate trust in the work we’re doing as an outside entity and to give us more information,” she says in the report.
In Washington state, Valley Communications 911 and Crisis Connections, a crisis support network, negotiated a pilot program that embeds 988 professionals in the 911 communications center. Members from both organizations told researchers they built a strong relationship through commitment to the goal and frequent meetings.
“It takes time to build relationships and trust. Go slow and smart and be intentional. Meet in different forums, build camaraderie and shared vision,” says Lora Ueland, former executive director of Valley Communications 911, in the report.
On the systemic level, the report’s authors stress the need for improved staffing and training for both workforces to avoid burnout. Many 911 call centers already operate at less than 50% of optimal staffing levels, according to data collected by the Health Lab.
While there were fears that the 988 hotline would draw dispatchers from the 911 workforce, that wasn’t the experience of those working in the industry.
One point of consensus was the need to address inconsistent training for 988 phone counselors. Some are hired without educational prerequisites. Some centers run their counselors through real 988 calls or extensive role play. Others receive no training before their first call.
“Crisis counselors are often recruited straight out of school or as volunteers and provided inadequate training to deal with life or death using zero physical cues,” one counselor told Crisis Crowd Founder Dan Fichter, who released a survey of 988 crisis counselors in 2024. “Throwing them to the sharks in crisis is unfair, not trauma-informed and downright dangerous.”
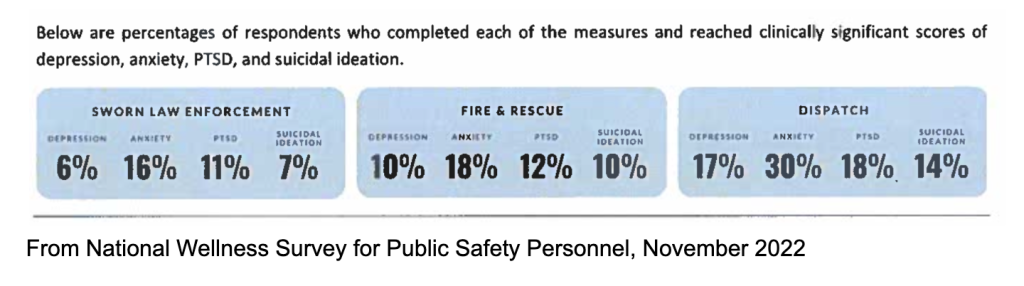
Burnout is especially high among 911 dispatchers, who are routinely exposed to primary and secondary trauma. A 2022 survey found that 911 dispatchers have significantly higher rates of depression, anxiety, PTSD, and suicidal ideation than law enforcement and firefighters, all of whom have higher rates of distress than the general public.
High levels of distress were also expressed by 988 phone counselors who responded to Fichter’s survey in 2023. Unlike 911 professionals, they are often answering calls exclusively from people experiencing a mental health crisis or those trying to help people in crisis.
“Most of the co-workers I started with left well before I did, and a number of crisis counselors I worked with experienced PTSD or severe burnout,” one counselor told Fichter.
The technology also presents challenges, including locating 988 callers when necessary; an inability to transfer some calls from 988 to 911 and vice versa; and privacy and statutory issues with data sharing.
Unlike people who call 911, callers to 988 aren’t tracked to a specific location to protect their privacy and to enable the service to roll out more quickly. With their location unknown, callers may feel more comfortable being open and asking for help.
Also, building a geolocation system like the 911 system, which was built to support landlines, not cell phones, is complex, expensive and time-consuming, according to the report.
Initially, this meant 988 calls were routed to call centers based on the area code of the phone, even if the caller was in a different state. In October 2024, the Federal Communications Commission created a rule requiring 988 calls to instead be georouted to the closest call center. In theory, this should improve access to local services for those calling, but more research is needed, according to the report.
While some systems can seamlessly transfer calls between 911 and 988, others require the caller to hang up and dial the other hotline. Some call centers offer their own unique solutions to this problem.
In Tucson, Arizona, fire, police and 988 all operate out of the same center. Call takers are also equipped with a speed dial to smoothly initiate a call transfer to others on staff. In Colorado, 911 operators can press a button to alert 988 calltakers that a transfer is being initiated.
To learn more about how the two systems can better collaborate, MindSite News reached out to the report authors with a few questions.
How do the various players involved in these systems — 911 and 988 dispatchers, police responders and mental health crisis responders — differ from each other? And how do the experts you consulted, the Inform988 Community of Practice, view the question of having callers’ phones be trackable via geolocation technology?
A common misconception is that 911 and law enforcement are interchangeable, when in reality they are two distinct functions. 911 professionals are tasked with gathering information to determine if an incident can be resolved over the phone, or if a police, fire, medical, or alternative response is needed.
One key difference between 911 and 988 is that the former hotline tracks the caller’s precise location while the latter does not, meaning that an in-person response to a 988 call cannot be as readily dispatched without the caller sharing their location.
The vast majority of calls to 988 are handled over the phone, but for the less than 2% that do involve deploying emergency services (often police), the (experts in the) Inform988 Community of Practice agreed that consent is key.
There is not a universal policy on gaining caller consent, but COPE members agreed that 988 call takers should clearly explain why they want to transfer the call. If the caller declines, then the call taker would not make the transfer unless they are required to by policy (i.e., if the caller is at imminent risk of harm to self or others.)
This is another area where communication and trust come into play – if 988 and 911 trust one another, and if community members trust that practitioners at both hotlines have their safety and well-being at heart, that provides the groundwork for both systems to function most effectively.
The report notes the importance of state advisory boards for crisis response systems. Why are these advisory boards so important and what can be done to ensure more states have them in place?
Each 988 and 911 center operates within its own local context, and state advisory boards can offer guidance, share information and resources, and develop standards for, among other things, coordination between 911 and 988, as has been done in California and Utah.
Gathering the relevant information can have a steep up-front cost, so having a statewide office tasked with that and disseminating it throughout the state can be very helpful in allowing each center to function at its best.
State level governing bodies can look at the existing advisory boards to learn how they came to be, what they have accomplished, and how they might be adapted to new states.
What can be done to ensure 988 can survive as long as 911 has?
As the crisis response landscape shifts and expands, the entities that provide the most needed services to people seeking relief from distress should be the ones to survive. More concretely, coordination between 988 and 911 can go a long way in ensuring the longevity of both.
Opioid overdoses continue downward trend in Oregon
Drug overdose deaths continued to plummet across the country in 2025, according to new data from the Centers for Disease Control and Prevention, falling 13.9% nationally from December 2024 to December 2025. The state with the biggest decline was Oregon, where overdose deaths fell by 35%.
North Carolina and New York also reduced their overdoses by more than 30%, according to data from the CDC.
It was the second year-over-year decline for Oregon, which previously had experienced seven straight years in which deadly overdoses rose. The decline is largely due to a reduction in fentanyl deaths, according to a new report from the Oregon Health Authority.
“We’re encouraged by these drops, but we can’t let up now,” Dr. Tom Jeanne, deputy state health officer and epidemiologist with the Oregon Health Authority, told Oregon Public Broadcasting. “Our overdose rates are still far above where they were five, six years ago.”
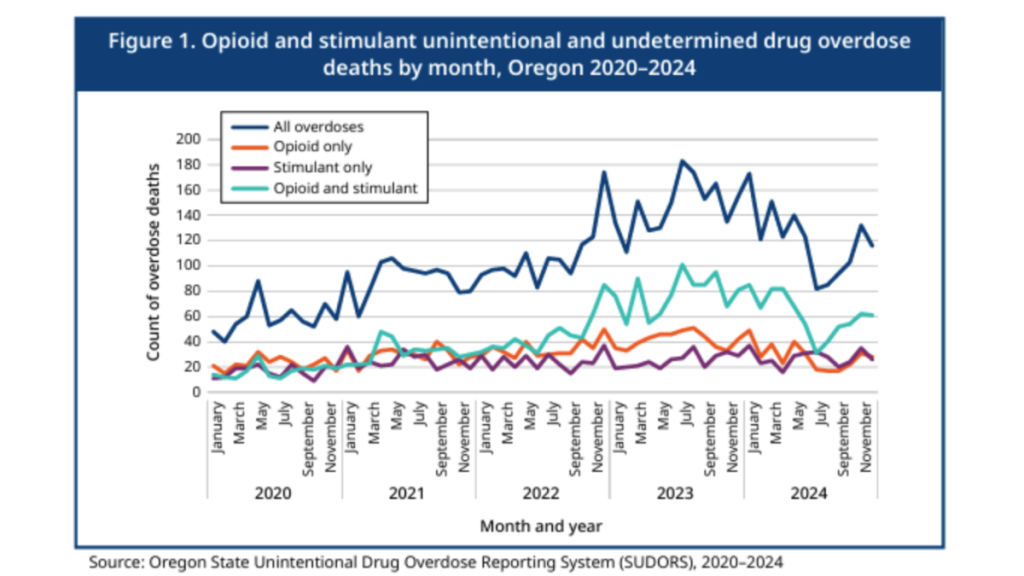
The trend matches what’s being seen in major cities across the country, where researchers are searching for explanations for the decline. Researchers at the Centers for Disease Control and Prevention suggested the rapid rise and fall of fatal overdoses was due to fentanyl’s saturation of the drug market.
Over the last decade, fentanyl transitioned from being an adulterant — an added ingredient in street drugs to reduce their cost and increase potency — to replacing commonly-used opioids like heroin, OPB reported.
“Fentanyl is so potent, about 100 times more potent than morphine, so it’s really dangerous for people who are not familiar with it,” Jeanne told OPB. “It takes a while for that to kind of ripple through and for users to become used to the changes.”
Learn more about the contributing factors here.
Until next month,
Josh McGhee
The name “MindSite News” is used with the express permission of Mindsight Institute, an educational organization offering online learning and in-person workshops in the field of mental health and wellbeing. MindSite News and Mindsight Institute are separate, unaffiliated entities that are aligned in making science accessible and promoting mental health globally.
Author

Related Articles

Film, Books and Streaming Series: Our Most Popular Arts and Culture Stories
From reviews of Succession and Seeing Red to the mental health benefits of fantasy fiction, we want to share some of our favorites.

Medical Cannabis Eases Agitation from Advanced Dementia
Agitation, including vocal outbursts or hitting, affects about half of patients with advanced dementia.
